Thalidomide, known by some as the most infamous drug in medical history, was revolutionary when initially released to the public (Stephens, Bunde and Fillmore, 2000). It was first introduced in Germany in 1956 as a sedative as well as a prevention method for symptoms of morning sickness for pregnant women (Calabrese and Resztak, 1998). Unknown to scientists and the general public, thalidomide caused abnormal fetal development, also known as teratogenic effects, the most notable being the shortening or absence of limbs (Ito, et al., 2010). How did what was formerly known as the safest drug on the market demolish the quality of life of so many newborns? The answer comes from understanding the stereochemistry of organic molecules.
Chemical compounds can have many different arrangements; these are referred to as stereoisomers (Valentová, et al., 2023). Stereoisomers can be broken down into two categories, diastereomers and enantiomers. Diastereomers do not appear as mirror images of each other whereas enantiomers appear as non-superimposable mirror images of one another (Lininger, et al., 2023). Enantiomers can also be referred to as chiral molecules due to the presence of a chiral center, a carbon atom bonded to four different groups. The only property that differentiates enantiomers from one another is the ability to rotate polarized light (Gal, 2002). A molecule that rotates light to the right is denoted as positive and a molecule that rotates light to the left is denoted as negative. Further, enantiomers can be identified as R and S according to the arrangement of groups around the chiral center. This property proves to be important when looking at the thalidomide crisis as one enantiomer is completely safe whereas the other has teratogenic effects (Figure 1) (Tokunaga, et al., 2018).

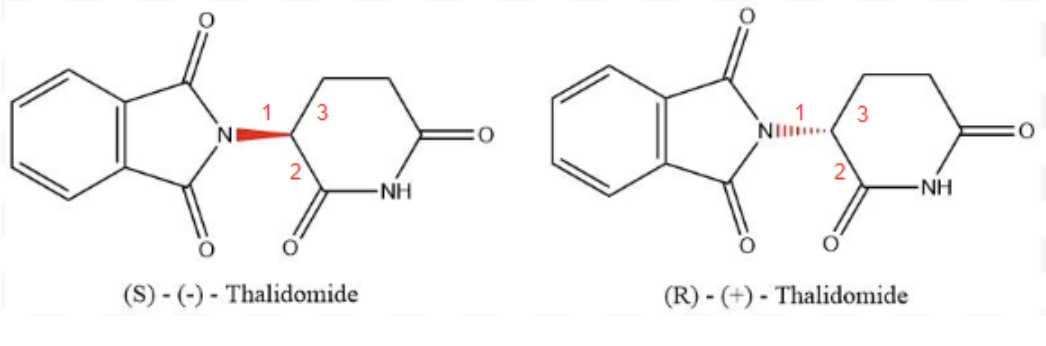
Figure 1. The two enantiomers of thalidomide. In red are the bonds that distinguish the enantiomers from each other changing how the molecule interacts with polarized light. The S-enantiomer has teratogenic effects whereas the R-enantiomer is safe. To identify each enantiomer, each substituent off of the chiral centre is given a priority based on the size of the substituent. If the substituent’s priority goes in a clockwise direction when the 4th priority substituent is into the page, it gets assigned R and if the substituent’s go in a counterclockwise direction, it gets assigned S (adapted from PubChem, 2023a; 2023b).
When released to the public, thalidomide enantiomers were not separated but instead were distributed in a racemic mixture consisting of a 50/50 mix of both R and S enantiomers (Tokunaga, et al., 2018). Initial trials were run using mice and rat in vivo models who did not experience the teratogenic effects that were seen in humans (Ito, et al., 2010). The exact mechanism of action of the S-enantiomer remained a scientific mystery for many years until in vivo zebrafish and chicken models were used to identify the primary target, the protein cereblon (CRBN). S-Thalidomide bonded to CRBN, decreasing levels of fibroblast growth factor (fgf8), an essential component of limb growth (Figure 2) (Shi and Chen, 2017). This causes the observed deformities in the limbs of individuals who were exposed to thalidomide in utero.

Figure 2. Thalidomide binding to CRBN protein causing teratogenic effects (Adapted from Fischer, et al., 2014).
While thalidomide has numerous negative effects on the human body, it has returned to the market as a treatment for certain incurable diseases such as erythema nodosum leprosum (ENL) (Bathula, et al., 2023). It inhibits tumour necrosis factor-a, proving to be the best treatment for ENL that is currently FDA-approved (Okafor, 2003). Thalidomide is also now used as a treatment for many other diseases if the individual receiving the treatment is not pregnant and is using multiple contraceptives to prevent future embryopathy (Annas and Elias, 1999).
The thalidomide crisis is one not to be forgotten as it demonstrates how small errors in science can have grave consequences for thousands of people. To avoid the crisis, perhaps FDA guidelines should have been stricter, or maybe scientists simply needed to go back to the basics of stereochemistry.
Works Cited
Annas, G.J. and Elias, S., 1999. Thalidomide and the Titanic: reconstructing the technology tragedies of the twentieth century. American Journal of Public Health, [online] 89(1), pp.98–101. https://doi.org/10.2105/AJPH.89.1.98.
Bathula, S., Sardana, K., Mathachan, S.R., Khurana, A., Ahuja, A. and Paliwal, P., 2023. A real-world study of low-dose thalidomide in severe erythema nodosum leprosum highlighting its mechanistic rationale in a resource-constrained target population. International Journal of Dermatology, [online] 62(1), pp.48–55. https://doi.org/10.1111/ijd.16315.
Calabrese, L. and Resztak, K., 1998. Thalidomide revisited: pharmacology and clinical applications. Expert Opinion on Investigational Drugs, [online] 7(12), pp.2043–2060. https://doi.org/10.1517/13543784.7.12.2043.
Fischer, E.S., Böhm, K., Lydeard, J.R., Yang, H., Stadler, M.B., Cavadini, S., Nagel, J., Serluca, F., Acker, V., Lingaraju, G.M., Tichkule, R.B., Schebesta, M., Forrester, W.C., Schirle, M., Hassiepen, U., Ottl, J., Hild, M., Beckwith, R.E.J., Harper, J.W., Jenkins, J.L. and Thomä, N.H., 2014. Structure of the DDB1–CRBN E3 ubiquitin ligase in complex with thalidomide. Nature, [online] 512(7512), pp.49–53. https://doi.org/10.1038/nature13527.
Gal, J., 2002. Single-Isomer Science: The Phenomenon and Its Terminology. CNS Spectrums, [online] 7(S1), pp.8–13. https://doi.org/10.1017/S1092852900028546.
Ito, T., Ando, H., Suzuki, T., Ogura, T., Hotta, K., Imamura, Y., Yamaguchi, Y. and Handa, H., 2010. Identification of a Primary Target of Thalidomide Teratogenicity. Science, [online] 327(5971), pp.1345–1350. https://doi.org/10.1126/science.1177319.
Lininger, A., Palermo, G., Guglielmelli, A., Nicoletta, G., Goel, M., Hinczewski, M. and Strangi, G., 2023. Chirality in Light–Matter Interaction. Advanced Materials, [online] 35(34), p.2107325. https://doi.org/10.1002/adma.202107325.
Okafor, M.C., 2003. Thalidomide for Erythema Nodosum Leprosum and Other Applications. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy, [online] 23(4), pp.481–493. https://doi.org/10.1592/phco.23.4.481.32115.
PubChem, 2023a. (+)-Thalidomide. [online] Available at: <https://pubchem.ncbi.nlm.nih.gov/compound/75792> [Accessed 11 November 2023].
PubChem, 2023b. (-)-Thalidomide. [online] Available at: <https://pubchem.ncbi.nlm.nih.gov/compound/92142> [Accessed 11 November 2023].
Shi, Q. and Chen, L., 2017. Cereblon: A Protein Crucial to the Multiple Functions of Immunomodulatory Drugs as well as Cell Metabolism and Disease Generation. Journal of Immunology Research, [online] 2017, p.9130608. https://doi.org/10.1155/2017/9130608.
Stephens, T.D., Bunde, C.J.W. and Fillmore, B.J., 2000. Mechanism of action in thalidomide teratogenesis. Biochemical Pharmacology, [online] 59(12), pp.1489–1499. https://doi.org/10.1016/S0006-2952(99)00388-3.
Tokunaga, E., Yamamoto, T., Ito, E. and Shibata, N., 2018. Understanding the Thalidomide Chirality in Biological Processes by the Self-disproportionation of Enantiomers. Scientific Reports, [online] 8(1), p.17131. https://doi.org/10.1038/s41598-018-35457-6.Valentová, J., Lintnerová, L., Miklášová, N., Oboňová, B. and Habala, L., 2023. Analogues of Anticancer Natural Products: Chiral Aspects. International Journal of Molecular Sciences, [online] 24(6), p.5679. https://doi.org/10.3390/ijms24065679.