Love can be thought of as the act of giving one’s heart, wholly and unshielded, to another and willingly losing emotional control. Although love has a temporary nature due to the temporality of life and the unpredictability of psychological changes associated with human growth, grief is the permanent remnant of love. In the extreme sense, however, Takotsubo cardiomyopathy (TTS or TCM), otherwise known as broken heart syndrome, is a type of acute heart failure that can result in death if left untreated (Sealove, Tiyyagura and Fuster, 2008). The Japanese word “takotsubo” refers to a traditional octopus trap with a shape resembling the affected left ventricle’s appearance during this condition (Assad et al., 2022). Typically preceded by emotional or physical stress, major triggers include the sudden loss of a loved one, natural disasters, an accident, financial or gambling losses, surgery, domestic abuse, relationship conflicts, extreme fright, or drug withdrawal (Khalid et al., 2023). The inability to identify the triggers of one-fourth of patients has made the syndrome’s etiology more difficult to decipher, but its prevalence in post-menopausal and elderly women aged 62-76 has been noted (Khalid et al., 2023).
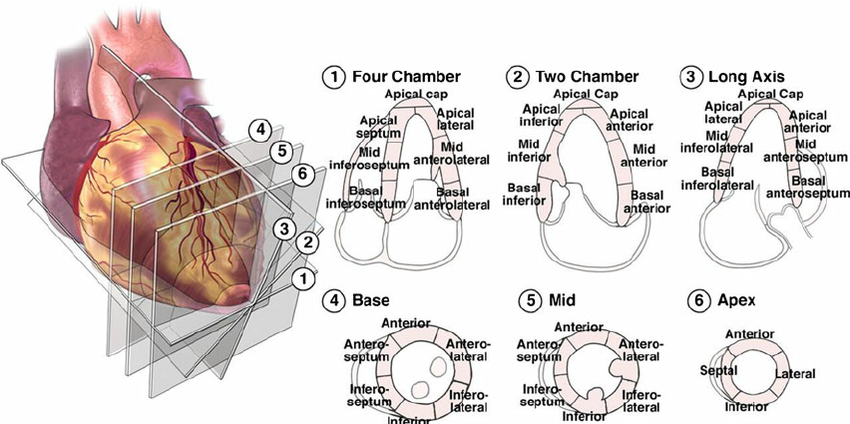
It is hypothesized that the individual perception of and response to triggers could play a more significant role in the onset of TTS than the nature of the triggers themselves. Studies show that chronic anxiety disorders are the most likely predisposing factor of TTS, with the reported prevalence of anxiety or depression being 56% and 48% in patients (Jenab et al., 2017). An observed trend is also that patients’ tendency not to share negative emotions that arise from stressful situations is positively correlated with exaggerated sympathetic and cardiovascular responses (Jenab et al., 2017). Considering both psychological and biochemical perspectives, patients’ resistance towards releasing emotional tension combined with somatizing tendencies render them susceptible to TTS. The syndrome is characterized by hypocontractility in one or more left ventricular (LV) segments, paired with hypercontractility in a relatively less impaired segment (Tranter and Lyon, 2018). Hypocontractility and hypercontractility are commonly observed in the apical and basal myocardia, respectively, but alternative TTS presentation with solely basal or mid-LV hypocontractility is possible (Tranter and Lyon, 2018). For reference, the heart wall consists of three muscular layers: the myocardium (middle), epicardium (outer), and the endocardium (inner). Left ventricular segmentation is pictured in Figure 1 to aid with visualization of TTS presentation.

Figure 1. Labeled left ventricular segments on echocardiographic views by the American Heart Association (Shalbaf et al., 2013).
Myocardial stunning arises when myocardial cells are overstimulated, causing abnormalities in heart wall motion and the consequent ventricular ballooning seen in TTS (Norcliffe-Kaufmann, 2023). The etiological hypothesis is that the adrenal medulla’s sudden secretion of catecholamines, such as norepinephrine, epinephrine, and dopamine, causes myocardial stunning. While the ballooning typically subsides with supportive care, atypicalities in the autonomic nervous system are frequently observed in survivors for years after the event (Norcliffe-Kaufmann, 2023). Common long-term dysfunctionalities include the heightened activation of the sympathetic nervous system by emotional and cognitive stressors or suppressed baroreflex sensitivity (Norcliffe-Kaufmann, 2023), the latter of which would disrupt the regulatory system illustrated in Figure 2.

Figure 2. Baroreflex physiological feedback mechanism that involves interactions between the nervous and cardiovascular systems (Shaffer and Meehan, 2020).
As illustrated in Figure 2, baroreceptors are located in the walls of specific blood vessels like the carotid sinus and aortic arch. Rises in blood pressure cause baroreceptors to signal the brain to decrease sympathetic nervous system activity and increase parasympathetic activity (Shaffer and Meehan, 2020). This results in a lower heart rate and relaxes blood vessels, thus reducing blood pressure. In contrast, when blood pressure (BP) drops, the baroreceptors increase BP by signaling to increase sympathetic activity and decrease parasympathetic activity to raise heart rate and constrict blood vessels (Shaffer and Meehan, 2020). TTS reduces the functionality of this feedback mechanism. This increases long-term susceptibility to conditions like hypertension (high blood pressure), orthostatic hypotension (abnormally low blood pressure upon standing), and other cardiovascular complications (Anderson, Little and Irving, 1990).
In alignment with the effects of long-term suppressed baroreflex sensitivity, a study conducted in Denmark on patients with first-time TTS from 2011 to 2018 concluded that TTS survivors have a 2.05 times higher risk of death and 4.24 times higher risk of hospitalization due to HF, compared with the background population (Butt et al., 2022). Nonetheless, data concerning long-term therapy for TTS recovery or prevention of TTS is scarce. Takotsubo syndrome should be further researched to determine what anatomically differentiates patients who make nearly full recoveries within two months and those who show persistent signs consistent with heart failure.
Works Cited
Anderson, I.D., Little, R.A. and Irving, M.H., 1990. An Effect of Trauma on Human Cardiovascular Control: Baroreflex Suppression. Journal of Trauma and Acute Care Surgery, 30(8), p.974.
Assad, J., Femia, G., Pender, P., Badie, T. and Rajaratnam, R., 2022. Takotsubo Syndrome: A Review of Presentation, Diagnosis and Management. Clinical Medicine Insights. Cardiology, 16, p.11795468211065782. https://doi.org/10.1177/11795468211065782.
Butt, J.H., Bang, L.E., Rørth, R., Schou, M., Kristensen, S.L., Yafasova, A., Havers-Borgersen, E., Vinding, N.E., Jessen, N., Kragholm, K., Torp-Pedersen, C., Køber, L. and Fosbøl, E.L., 2022. Long-term Risk of Death and Hospitalization in Patients With Heart Failure and Takotsubo Syndrome: Insights From a Nationwide Cohort. Journal of Cardiac Failure, 28(10), pp.1534–1544. https://doi.org/10.1016/j.cardfail.2022.02.002.
Khalid, N., Ahmad, S.A., Shlofmitz, E. and Chhabra, L., 2023. Pathophysiology of Takotsubo Syndrome. In: StatPearls. [online] Treasure Island (FL): StatPearls Publishing. Available at: <http://www.ncbi.nlm.nih.gov/books/NBK538160/>
Norcliffe-Kaufmann, L., 2023. Chapter 85 – Myocardial stunning and takotsubo cardiomyopathy. In: I. Biaggioni, K. Browning, G. Fink, J. Jordan, P.A. Low and J.F.R. Paton, eds. Primer on the Autonomic Nervous System (Fourth Edition). [online] Academic Press. pp.489–494. https://doi.org/10.1016/B978-0-323-85492-4.00054-5.
Obunai, K., Misra, D., Van Tosh, A. and Bergmann, S.R., 2005. Metabolic evidence of myocardial stunning in takotsubo cardiomyopathy: A positron emission tomography study. Journal of Nuclear Cardiology, 12(6), pp.742–744. https://doi.org/10.1016/j.nuclcard.2005.06.087.
Sealove, B.A., Tiyyagura, S. and Fuster, V., 2008. Takotsubo Cardiomyopathy. Journal of General Internal Medicine, 23(11), pp.1904–1908. https://doi.org/10.1007/s11606-008-0744-4.
Shaffer, F. and Meehan, Z.M., 2020. A Practical Guide to Resonance Frequency Assessment for Heart Rate Variability Biofeedback. Frontiers in Neuroscience, [online] 14. Available at: <https://www.frontiersin.org/journals/neuroscience/articles/10.3389/fnins.2020.570400>
Shalbaf, A., Behnam, H., Alizade-Sani, Z. and Shojaeifard, M., 2013. Automatic Classification of Left Ventricular Regional Wall Motion Abnormalities in Echocardiography Images Using Nonrigid Image Registration. Journal of digital imaging : the official journal of the Society for Computer Applications in Radiology, 26. https://doi.org/10.1007/s10278-012-9543-x.
Tranter, M.H. and Lyon, A.R., 2018. Takotsubo Syndrome. In: R.S. Vasan and D.B. Sawyer, eds. Encyclopedia of Cardiovascular Research and Medicine. [online] Oxford: Elsevier. pp.533–536. https://doi.org/10.1016/B978-0-12-809657-4.10913-5.