While there are many instances in which synchronicity may be beneficial, such as musicians playing in unison, the same cannot always be said for neurons in the brain. A seizure results from atypical, hypersynchronous electrical activity in the brain (Milligan, 2021). Neurons become overexcited and fire in abnormal patterns, often recruiting neighboring neurons to fire in unison. This overactive state may be produced by excitation in neuronal pathways, a loss of inhibitory networks that normally regulate neuronal firing, or both. Repeated, unprovoked seizures result in diagnosis of epilepsy (Milligan, 2021).
A focal onset seizure is a common type of seizure characterized by abnormal neuronal activity in a localized brain region, which often produces abnormal behaviour of a particular limb (Milligan, 2021). Epilepsy treatment typically begins with the use of anti-epileptic drugs, selected to suit the patient’s seizure type; however, about 30% of epilepsy cases, especially focal epilepsy, are drug-resistant (Milligan, 2021; Toffa et al., 2020). Vagus nerve stimulation (VNS), a neuromodulation-based intervention, presents a viable alternative.
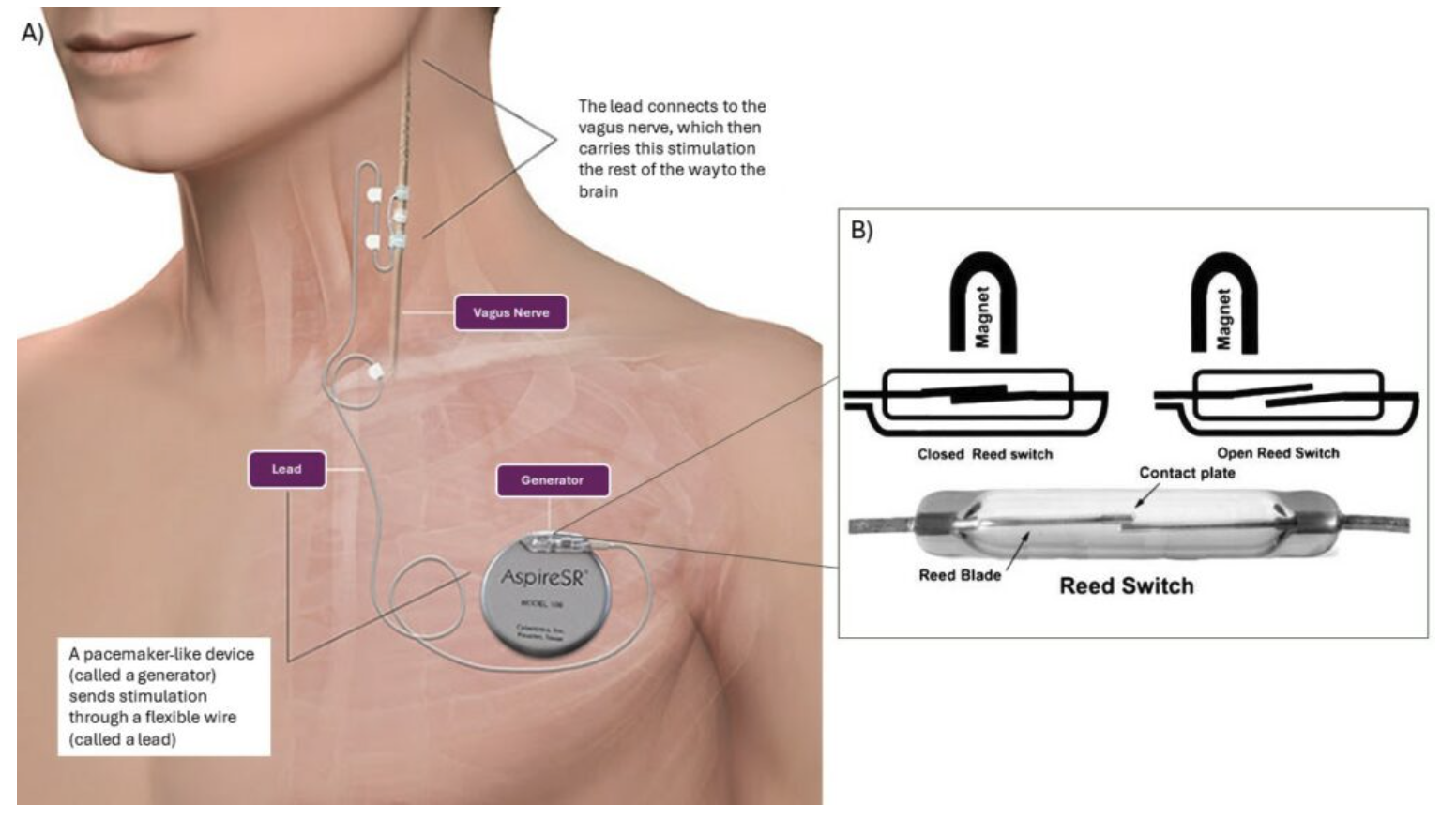
VNS involves the implantation of a battery-powered device (Figure 1A) to deliver controlled stimulation to the vagus nerve (González, Yengo-Kahn and Englot, 2019; Carron et al., 2023). This nerve contains nerve fibers belonging to the sympathetic nervous system, otherwise known as the body’s ‘fight or flight’ mechanism. VNS is thought to produce numerous effects which can prevent or arrest an epileptic seizure (Carron et al., 2023). It is primarily prescribed for focal onset seizures, in which patients usually retain consciousness, allowing them to activate the device (Toffa et al., 2020). When an individual or caregiver recognizes the onset of a seizure, they may initiate electrical stimulation using a magnet and reed switch (Figure 1B) or an external programming device (Kwan et al., 2010; Afra et al., 2021).

Stimulation parameters including pulse width, current intensity, frequency, on-off time, and duration of the stimulus are all modifiable through VNS (Figure 3). Increasing the current output rarely improves results, while there are also many inter-individual variations in terms of the appropriate pulse width, output current and even electrode design (Carron et al., 2023). The typical stimulation range implemented is 20-30 Hz, with a pulse duration of less than 500 microseconds, alternating On periods of 30-90 seconds with Off periods of five minutes (Toffa et al., 2020).

Despite reducing seizure frequency and improving quality of life for many users, VNS is not effective in all epilepsy patients, and its mechanism remains to be fully elucidated (González, Yengo-Kahn and Englot, 2019; Carron et al., 2023). A recent review of the mechanism of VNS suggests numerous explanations for its efficacy, including increasing the release of the neurotransmitter noradrenaline, and reducing the connectivity of neurons in brain regions producing focal seizures (Carron et al., 2023). Some patients are unresponsive to VNS; however, this allows researchers to study biological differences between responders and non-responders to help elucidate the mechanism of VNS (Carron et al., 2023).
VNS offers a unique alternative to traditional forms of epilepsy treatment and has successfully helped numerous patients manage their epilepsy. As the technology improves, devices become more responsive and offer more stimulation parameters to treat the diverse needs of epilepsy patients. VNS provides the security of having an immediate response to the onset of a seizure, improving the lives of both patients and caregivers tackling the challenge of epilepsy.
References
Afra, P., Adamolekun, B., Aydemir, S. and Watson, G.D.R., 2021. Evolution of the Vagus Nerve Stimulation (VNS) Therapy System Technology for Drug-Resistant Epilepsy. Frontiers in Medical Technology, [online] 3. Available at: <https://www.frontiersin.org/articles/10.3389/fmedt.2021.696543> [Accessed 18 February 2024].
Carron, R., Roncon, P., Lagarde, S., Dibué, M., Zanello, M. and Bartolomei, F., 2023. Latest Views on the Mechanisms of Action of Surgically Implanted Cervical Vagal Nerve Stimulation in Epilepsy. Neuromodulation: Technology at the Neural Interface, 26(3), pp.498–506. https://doi.org/10.1016/j.neurom.2022.08.447.
González, H.F.J., Yengo-Kahn, A. and Englot, D.J., 2019. Vagus Nerve Stimulation for the Treatment of Epilepsy. Neurosurgery Clinics of North America, 30(2), pp.219–230. https://doi.org/10.1016/j.nec.2018.12.005.
Jacob, S., Panaich, S.S., Maheshwari, R., Haddad, J.W., Padanilam, B.J. and John, S.K., 2011. Clinical applications of magnets on cardiac rhythm management devices. EP Europace, 13(9), pp.1222–1230. https://doi.org/10.1093/europace/eur137.
Kwan, P., Arzimanoglou, A., Berg, A.T., Brodie, M.J., Allen Hauser, W., Mathern, G., Moshé, S.L., Perucca, E., Wiebe, S. and French, J., 2010. Definition of drug resistant epilepsy: Consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia, 51(6), pp.1069–1077. https://doi.org/10.1111/j.1528-1167.2009.02397.x.
Milligan, T.A., 2021. Epilepsy: A Clinical Overview. The American Journal of Medicine, 134(7), pp.840–847. https://doi.org/10.1016/j.amjmed.2021.01.038.
Royal Children’s Hospital, 2024. [image online] Available at: https://www.rch.org.au/neurology/patient_information/vagus_nerve_stimulation/ [Accessed 7 March, 2024].
Thompson, S.L., O’Leary, G.H., Austelle, C.W., Gruber, E., Kahn, A.T., Manett, A.J., Short, B. and Badran, B.W., 2021. A Review of Parameter Settings for Invasive and Non-invasive Vagus Nerve Stimulation (VNS) Applied in Neurological and Psychiatric Disorders. Frontiers in Neuroscience, [online] 15. Available at: <https://www.frontiersin.org/journals/neuroscience/articles/10.3389/fnins.2021.709436> [Accessed 18 February 2024].
Toffa, D.H., Touma, L., El Meskine, T., Bouthillier, A. and Nguyen, D.K., 2020. Learnings from 30 years of reported efficacy and safety of vagus nerve stimulation (VNS) for epilepsy treatment: A critical review. Seizure, 83, pp.104–123. https://doi.org/10.1016/j.seizure.2020.09.027.