Multiple studies conducted in the 1980s and 1990s concluded that up to 80% of patients who received psychiatric treatment were misdiagnosed (Klonoff & Landrine, 1997). Diagnostic shadowing is the attribution of a person’s symptoms to a psychiatric illness without testing for the potential existence of underlying physical disorders (Happell, et al., 2016). Frequent diagnostic errors waste the time and money of both patients and physicians while neglecting undetected, potentially lethal physical disorders. The direct costs of psychiatric treatment include healthcare costs like medication, physician visits, and hospitalization. The fees associated with productivity loss and misallocated treatment only worsen the financial burden of seeking care (Trautmann, et al., 2016).
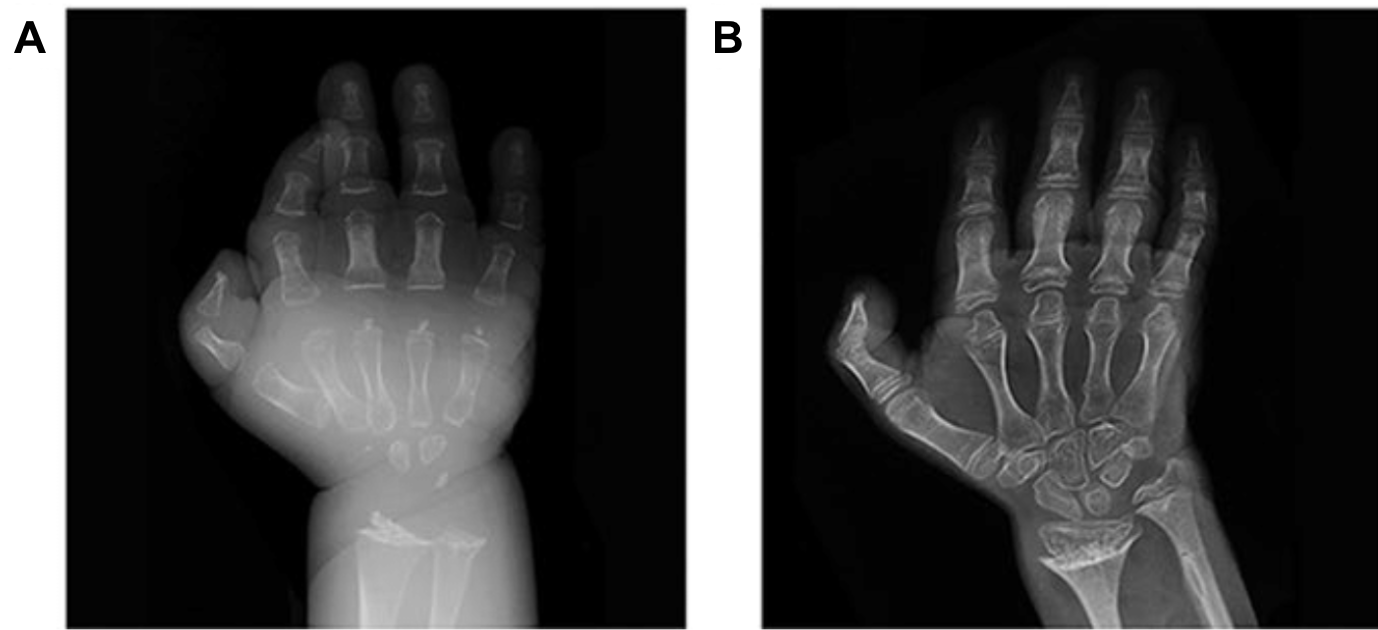
Common physical illnesses that present with primarily psychological symptoms include thyroid disorders, sleep apnea, and neurological disorders like Parkinson’s disease (Stanford, et al., 2020). Before an understanding of the pathophysiology of hypothyroidism was established around 1886, patients with mental and physical sluggishness were diagnosed as depressed without hesitation. In reality, the lack of sufficient triiodothyronine and thyroxine production by an under-active thyroid gland was the cause behind patients’ decreased anatomical functionality (Stanford, et al., 2020). When left untreated, hypothyroidism can cause a lack of bone development, as seen in Figure 1 below, in addition to goiters, atherosclerosis, permanent brain damage, infertility, and myxedema comas that require emergency medical treatment (Duncan Bassett & Williams, 2018). Despite present-day knowledge about overlapping symptoms between hypothyroidism and psychosis, physical examinations are often improperly conducted as providers interpret all observed concerns as symptoms of the mental health diagnosis. This phenomenon where mental health issues frame consumer-provider relationships is known as “symptomising” (Happell, et al., 2016). Providers fall into the trap of over-reliance on psychotropic medication and pursue the belief that higher dosages are needed when desired improvements in health are not observed. This is unhealthy, unhelpful, and financially detrimental for patients.

Temporal lobe epilepsy (TLE) is the most common seizure disorder, affecting around 71% of the 70 million people who suffer from epilepsy worldwide (McIntosh & Das, 2023). However, TLE presents without convulsions, but rather with behavioral problems, cognitive impairment, psychosis, and personality shifts. Due to the overlap of the aforementioned symptoms with bipolar disorder (BD), misdiagnosis of TLE as BD is often not caught for extensive time periods (Klonoff & Landrine, 1997). Without treatment, repeated temporal lobe seizures can cause hippocampus shrinkage, which may cause memory and mood issues in addition to an increased risk of sudden unexpected death in epilepsy (McIntosh & Das, 2023). Increased focus on symptoms inconsistent with the initial diagnosis can help identify the diagnostic tests needed to evaluate alternative conceptualizations of a patient’s problem. Additionally, patients with acute psychiatric symptoms should be examined by both psychiatrists and neurologists. When rapid fluctuations in behaviour or mood, muscle cramps, or stereotypical seizure-like symptoms are observed in patients, conducting electroencephalograms would allow a definitive conclusion about the potential diagnosis of epilepsy to be reached before the recommendation of therapy or psychiatric medication (Sand, et al., 2013).
Ultimately, increased collaboration between physical and mental health practitioners through educational interventions and general destigmatization would allow more thorough assessments to be conducted, preventing the development of long-term adverse effects. If a physician has taken all the correct measures to treat a problem and is unable to do so, they likely have the wrong issue in mind.
References
Duncan Bassett, J.H. and Williams, G.R., 2018. Analysis of physiological responses to thyroid hormones and their receptors in bone. Methods in Molecular Biology, 1801, pp.123–154. 10.1007/978-1-4939-7902-8_12
Happell, B., Ewart, S.B., Bocking, J., Platania‐Phung, C. and Stanton, R., 2016. ‘That red flag on your file’: Misinterpreting physical symptoms as mental illness. Journal of Clinical Nursing, 25(19–20), pp.2933–2942. 10.1111/jocn.13355
Klonoff, E.A. and Landrine, H., 1997. Preventing misdiagnosis of women: A guide to physical disorders that have psychiatric symptoms. London: SAGE Publications.
McIntosh, W.C. and Das, J.M., 2023. Temporal seizure. [online] National Library of Medicine. Available at: <https://www.ncbi.nlm.nih.gov/books/NBK549852/> [Accessed 2 Nov. 2023].
Sand, T., Bjørk, M.H. and Vaaler, A.E., 2013. Is EEG a useful test in adult psychiatry? Tidsskrift for Den norske legeforening, 133, pp.1200–1204. 10.4045/tidsskr.12.1253
Stanford, D., Ling, C., Rodney, T. and Shattell, M., 2020. Mental illness misdiagnosed: Increasing awareness of obscure physical illnesses. Journal of Psychosocial Nursing and Mental Health Services, 58(10), pp.2–3. 10.3928/02793695-20200814-02
Trautmann, S., Rehm, J. and Wittchen, H., 2016. The economic costs of mental disorders. EMBO Reports, 17(9), pp.1245–1249. 10.15252/embr.201642951