Chronic illness can be incredibly debilitating both mentally and physically and can really take a toll on an individual’s quality of life. Youth with inflammatory bowel disease (IBD) including ulcerative colitis and Crohn’s disease, deal with pain on a day to day basis (Szigethy, et al., 2017). Essentially, IBD causes inflammation in the digestive tract, and this can result in symptoms such as abdominal pain, fatigue, diarrhea, bloody stool, malnutrition, loss of appetite, and joint pain (Ku & Mahadevan, 2022).
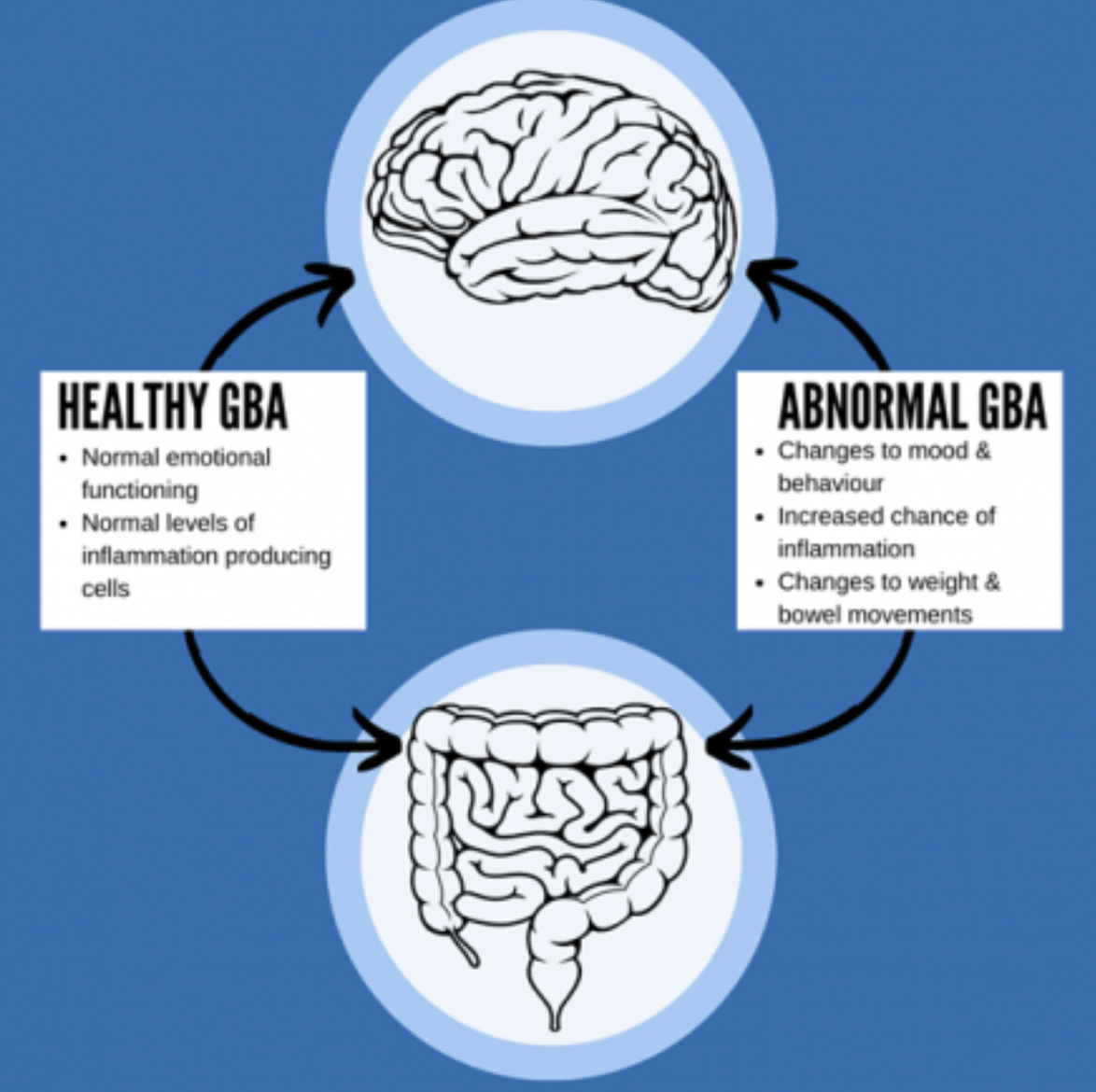
Inflammatory bowel disease and mental health are complex and deeply connected. In fact, around 50% of youth with IBD also deal with psychiatric disorders, therefore the correlation between IBD and mental health issues is the highest of all chronic illnesses (Engstrom, 1999). Children with IBD tend to struggle with accepting their disease because they find the symptoms embarrassing, which causes them to struggle with accepting and discussing their disease for fear of judgment (Engstrom, 1999; Qualter, et al., 2020). This type of coping mechanism may lead to the onset of depression, loneliness, and anxiety, and inversely, as disease symptoms get more severe, a child’s mental health symptoms are also negatively affected (Figure 1) (Gray, et al., 2015).

Physical symptoms may be better managed by learning to target the mental health aspect of IBD. For optimal care to be delivered, the practitioner must explain the interconnected mechanisms behind the mind-body connection to the patient and their family (Szigethy, et al., 2017). An emotionally intelligent practitioner allows for both the patient to be understood, and for the family to act as a better support system for their child. By creating a safe space for the youth, they are able to open up about their struggles more and slowly erase the stigma around the disease. Also, a child is able to manage their stressors better when they have a support system such as their family to fall back onto when needed (Gray, et al., 2015). Further, a screening process may be implemented by a healthcare practitioner, to make sure that mental health symptoms in IBD patients are not neglected or overlooked (Szigethy, et al., 2017). By learning to target the mental health aspect of IBD, physical symptoms may be better managed (Stapersma, et al., 2019).
Overall, by teaching youth with IBD how to be vulnerable with their mental health and offering the most integrated care possible, they can learn to value both their physical and mental health in the future. Transitioning from childhood to adulthood is already a difficult process, and IBD amplifies the difficulty (Stapersma, et al., 2019). Milestones that occur during this transition period, such as finding a job, going to parties with friends, going away for college, becoming independent from family, and building long-term relationships may be affected by IBD (Stapersma, et al., 2019). In turn, this can especially impact mental health and cause a child to struggle with their perception of themselves and their disease. These extra layers of challenges call for care that accounts for mental health aspects and does not dismiss them.
With integrated care, youth are able to grow on a strong foundation and better understand who they are. All in all, this prioritization of mental and physical wellbeing allows youth to more easily transition from child to adult care.
References:
Gray, W.N. et al. (2015) “Health-related quality of life in youth with Crohn disease,” Journal of Pediatric Gastroenterology & Nutrition, 60(6), pp. 749–753. Available at: https://doi.org/10.1097/mpg.0000000000000696.
Engström, I. (1999). “Inflammatory Bowel Disease in Children and Adolescents: Mental Health and Family Functioning,” Journal of Pediatric Gastroenterology and Nutrition, 28 (Supplement), S28–S33. Available at: https://doi.org/10.1097/00005176-199904001-00004
Qualter, P. et al. (2020) “Depression, anxiety, and loneliness among adolescents and young adults with IBD in the UK: The role of disease severity, age of onset, and embarrassment of the condition,” Quality of Life Research, 30(2), pp. 497–506. Available at: https://doi.org/10.1007/s11136-020-02653-9.
Ku, F. and Mahadevan, U. (2022) Inflammatory bowel disease, Inflammatory bowel disease | Office on Women’s Health. Available at: https://www.womenshealth.gov/a-z-topics/inflammatory-bowel-disease (Accessed: March 8, 2023).
Stapersma, L., et al. (2019). “Psychological outcomes of a cognitive behavioral therapy for youth with inflammatory bowel disease: Results of the happy-IBD randomized controlled trial at 6- and 12-month follow-up,” Journal of Clinical Psychology in Medical Settings, 27(3), 490–506. Available at: https://doi.org/10.1007/s10880-019-09649-9
Szigethy, E. M., et al. (2017). White Paper Aga: The impact of mental and psychosocial factors on the care of patients with inflammatory bowel disease. Clinical Gastroenterology and Hepatology, 15(7), 986–997. https://doi.org/10.1016/j.cgh.2017.02.037
Turner, K. (2021) Mental health and the gut-brain axis, Encounter Youth. Available at: https://www.encounteryouth.com.au/you-got-this/mental-health-and-the-gut-brain-axis/ (Accessed: March 1, 2023).