There are many layers within the skull that protect the brain from injuries, but is there an organism that can worm its way into the brain. Neurocysticercosis (NC) is caused by an infection of the larval cystic form of Taenia solium in the central nervous system (CNS) (Gripper and Welburn, 2017). It is one of the most common CNS-related parasitic diseases worldwide. Despite this, it is on the World Health Organization list of neglected diseases (Gripper and Welburn, 2017). Neurocysticercosis typically affects low-income countries in Asia, South America, and Africa; however, through migration, this disease is prevalent worldwide (Butala, et al., 2021). It is one of the leading causes of human epilepsy in low-income regions (Butala, et al., 2021).
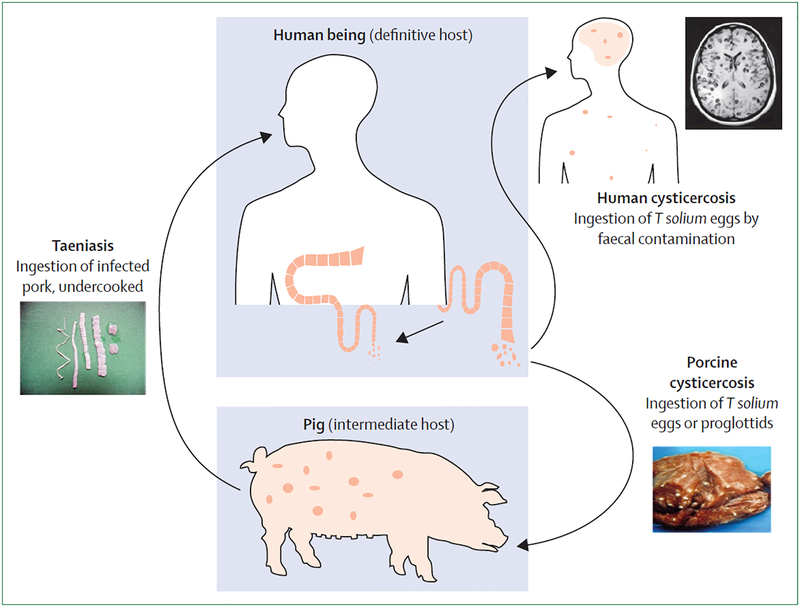
Neurocysticercosis typically occurs in regions with poor sanitation and free-roaming animals (El-Kady, et al., 2021). Once pigs ingest Taenia solium eggs through exposure to infested human feces, the embryos are transported through the bloodstream and carried to peripheral tissues. Subsequently, digestive enzymes help the embryos mature into cysticerci, which are made up of a vesicular wall and a scolex (main body). Once T. solium enters the brain in its vesicular form, it can survive for several years (El-Kady, et al., 2021). Pigs then become an intermediate host, until humans ingest undercooked pork which is infested with T. solium cysts and become the definitive host (Figure 1) (Garcia, Nash and Del Brutto, 2014). The cysts enter humans and develop into mature tapeworms in the brain (Nash, et al., 2015). The tapeworms reside in the small intestine by attaching themselves to the intestinal walls with suckers and hooks. They shed eggs that are excreted from the body through feces, and the cycle repeats when pigs are exposed to the human feces (Nash, et al., 2015).

Parasites can enter the brain parenchyma (functional layer of tissue in the brain), ventricular system, or spinal cord inside the nervous system (Brutto, 2014). This can lead to a number of issues like focal neurologic deficits, intracranial hypertension, and decline in cognition (Brutto, 2014). Typically, NC cannot be diagnosed histologically, and neuroimaging is required to confirm the presence and stage of involution of the cysticerci (Figure 2) (Rajshekhar, 2016). This poses a significant issue, as neuroimaging techniques are expensive and often inaccessible to populations that regularly experience cases of NC. Diagnosis methods also include serological testing, which detects anti- T. solium antibodies in the blood, urine, and CNS (Butala, et al., 2021). Furthermore, treatment of NC includes anti-epileptic drugs, corticosteroids for inflammation, and anthelminthic medications to eradicate cysts; however, the effectiveness of these treatments is inconclusive (Nash and Garcia, 2011).

Neurocysticercosis is preventable through implementation of proper sanitation (Brutto, 2014). Eradication programs can be implemented, but must target the tapeworms at all stages of their lifecycles in the environment to avoid a reemergence in prevalence (Brutto, 2014). Eradication is also difficult due to the high number of asymptomatic patients (Carpio, et al., 2018).
Currently there are no effective treatments or cures for this disease, rather treatments are focused on short-term relief. Eradication is seemingly the most effective plan of action for this disease; however since NC affects low-income countries, there are barriers in implementing eradication programs. Since NC is a global parasitic CNS disease, it is important to encourage research into feasible treatment options to alleviate the health burden NC poses on low- and middle-income countries.
Bibliography
Brutto, O.H.D., 2014. Neurocysticercosis. The Neurohospitalist, 4(4), pp.205–212. https://doi.org/10.1177/1941874414533351.
Butala, C., Brook, T.M., Majekodunmi, A.O. and Welburn, S.C., 2021. Neurocysticercosis: Current Perspectives on Diagnosis and Management. Frontiers in Veterinary Science, [online] 8. https://doi.org/10.3389/fvets.2021.615703.
Carpio, A., Fleury, A., Romo, M.L. and Abraham, R., 2018. Neurocysticercosis: the good, the bad, and the missing. Expert Review of Neurotherapeutics, 18(4), pp.289–301. https://doi.org/10.1080/14737175.2018.1451328.
El-Kady, A.M., Allemailem, K.S., Almatroudi, A., Abler, B. and Elsayed, M., 2021. Psychiatric Disorders of Neurocysticercosis: Narrative Review. Neuropsychiatric Disease and Treatment, 17, pp.1599–1610. https://doi.org/10.2147/NDT.S306585.
Garcia, H.H., Nash, T.E. and Del Brutto, O.H., 2014. Clinical symptoms, diagnosis, and treatment of neurocysticercosis. The Lancet Neurology, 13(12), pp.1202–1215. https://doi.org/10.1016/S1474-4422(14)70094-8.
Gripper, L.B. and Welburn, S.C., 2017. The causal relationship between neurocysticercosis infection and the development of epilepsy – a systematic review. Infectious Diseases of Poverty, 6(1), p.31. https://doi.org/10.1186/s40249-017-0245-y.
Li, X.-D., Wang, H.-B., Zhou, H., Zhou, A.-N., Zhao, L., Liu, Y.-H., Gong, X.-Q. and Zhang, X.-H., 2016. Good recovery of a patient with neurocysticercosis using two antihelminthic drugs combined with steroid. Neuroimmunology and Neuroinflammation, 3, pp.120–123. https://doi.org/10.20517/2347-8659.2015.51.
Nash, T.E. and Garcia, H.H., 2011. Diagnosis and treatment of neurocysticercosis. Nature Reviews Neurology, 7(10), pp.584–594. https://doi.org/10.1038/nrneurol.2011.135.
Nash, T.E., Mahanty, S., Loeb, J.A., Theodore, W.H., Friedman, A., Sander, J.W., Singh, G., Cavalheiro, E., Del Brutto, O.H., Takayanagui, O.M., Fleury, A., Verastegui, M., Preux, P.-M., Montano, S., Pretell, E.J., White Jr, A.C., Gonzales, A.E., Gilman, R.H. and Garcia, H.H., 2015. Neurocysticercosis: A natural human model of epileptogenesis. Epilepsia, 56(2), pp.177–183. https://doi.org/10.1111/epi.12849.
Rajshekhar, V., 2016. Neurocysticercosis: Diagnostic problems & current therapeutic strategies. The Indian Journal of Medical Research, 144(3), pp.319–326. https://doi.org/10.4103/0971-5916.198686.