
High phosphorus levels in patients with chronic kidney disease (CKD) have been directly related to increased mortality rates (Figure 1)(Noori et al. 2010). In CKD patients experiencing progressive loss of kidney function, a phosphorus-restricted diet is often a management method for hyperphosphatemia. In this condition, net intestinal absorption exceeds renal excretion and/or dialysis removal of waste, resulting in excess phosphate (phosphorus) in the bloodstream (D’Alessandro et al. 2015). Hyperphosphatemia increases the risk of vascular calcification, leading to heart attack, stroke, and death in CKD patients(Cleveland Clinic, n.d.). Because conventional medical interventions like dialysis are often insufficient to clear this mineral load, the therapeutic focus must shift to strictly limiting dietary intake. However, the efficacy of this clinical intervention is fundamentally compounded by systemic issues of food-industry transparency and the social determinants of health.
Dietary phosphorus is consumed in two distinct forms: as naturally occurring organic phosphorus or as inorganic preservative additives (D’Alessandro et al., 2015). On average, only 40-60% of organic phosphorus in natural food components is absorbed. Conversely, the absorption of inorganic phosphorus added as food preservatives can reach upwards of 100% due to key differences in bioavailability between phosphorus from natural and highly processed foods. Hence, the role of diet is paramount in controlling phosphorus load in CKD patients to prevent serious health risks (Ritz et al. 2012).
Composition and bioavailability of organic phosphates differ in their origin (Figure 2); plant-derived organic phosphates (beans, nuts, whole grains, etc) are in the form of phytates, while animal-derived organic phosphates (meat, eggs, dairy, etc) are bound to proteins, phospholipids, and nucleic acids (Wagner 2023). The bioavailability of phosphate from phytates is low, as humans lack sufficient phytase enzymatic activity to cleave the phosphorus from the phytate complex; the mineral cannot be fully freed for absorption in the digestive tract (20-50% absorption) (Dunford and Calvo 2025). Conversely, animal-derived organic phosphates are bound to digestible organic molecules. Digestive enzymes in the gastrointestinal tract (alkaline phosphatases) can hydrolyze these compounds to release free inorganic phosphate ions, which are then absorbed into the bloodstream (40-60% absorption) (Wagner 2023). With organic phosphates found in natural foods requiring additional enzymatic activity to release inorganic phosphate, absorption is limited, preventing hyperphosphatemia.
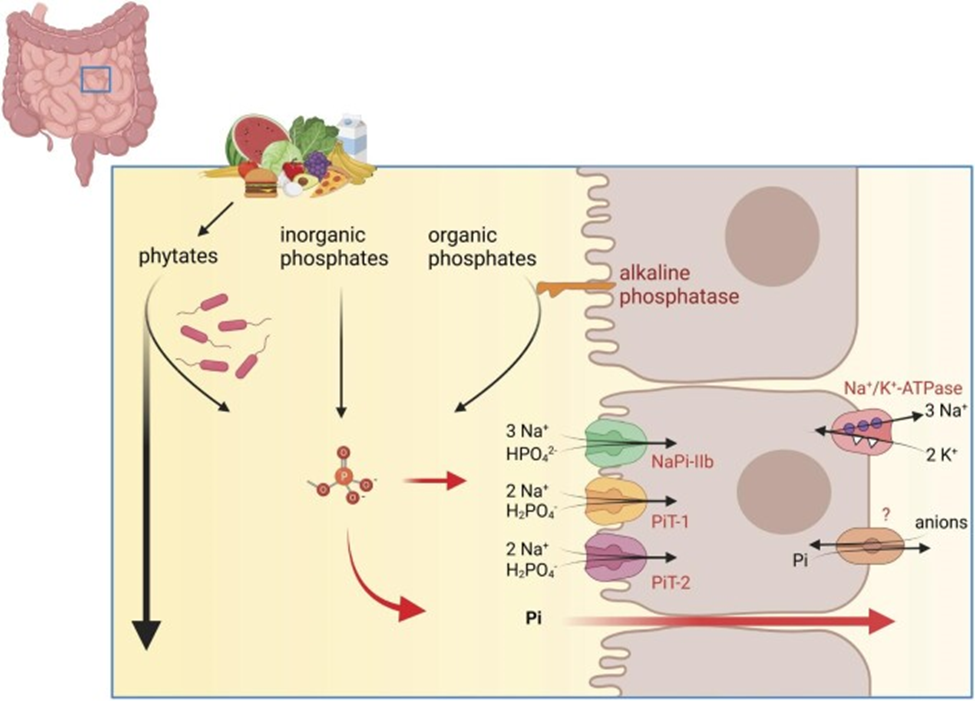
Inorganic phosphates are free phosphate salts that are in a nonorganically bound form. Thus, they bypass enzymatic breakdown and are absorbed more readily (100%) via active transport and paracellular passive driving forces (Wagner 2023). Inorganic phosphates are used as food additives in the majority of processed foods, with over 50,000 food products in the United States containing one or more phosphate additives; this includes fast food and restaurants. Under nutrition ingredient labels, these additives can typically appear as lecithin, sodium phosphate, calcium phosphate, modified starches, and sodium acid pyrophosphate (Dunford and Calvo 2025).
While transitioning to a diet of whole, organic foods appears to be a straightforward clinical solution, implementation is hindered by socioeconomic disparities that limit affordable organic food access for low-income populations, alongside a lack of regulatory mandates requiring companies to label the highly bioavailable inorganic phosphorus hidden in affordable, processed food (Borgi 2019, Gutiérrez et al. 2010). Ultimately, managing phosphorus in CKD is not merely a matter of biological understanding, but a complex challenge that requires both enhanced regulatory transparency in the food industry and equitable access to the whole-food diets necessary for patient survival.
References
Borgi, Lea. 2019. “Inclusion of Phosphorus in the Nutrition Facts Label.” Clinical Journal of the American Society of Nephrology : CJASN 14 (1): 139–40. https://doi.org/10.2215/CJN.07230618.
Cleveland Clinic. n.d. “Hyperphosphatemia: Causes, Symptoms & Treatment.” Accessed January 7, 2026. https://my.clevelandclinic.org/health/diseases/24293-hyperphosphatemia.
D’Alessandro, Claudia, Giorgina B Piccoli, and Adamasco Cupisti. 2015. “The ‘Phosphorus Pyramid’: A Visual Tool for Dietary Phosphate Management in Dialysis and CKD Patients.” BMC Nephrology 16 (January): 9. https://doi.org/10.1186/1471-2369-16-9.
Dunford, Elizabeth K, and Mona S Calvo. 2025. “Phosphate-Based Additives in Processed Foods: Is Excess Exposure a Cause for Concern? A Cross-Sectional Examination of the United States Packaged Food Supply.” The American Journal of Clinical Nutrition 121 (4): 873–81. https://doi.org/10.1016/j.ajcnut.2025.01.009.
Gutiérrez, Orlando M., Cheryl Anderson, Tamara Isakova, et al. 2010. “Low Socioeconomic Status Associates with Higher Serum Phosphate Irrespective of Race.” Journal of the American Society of Nephrology : JASN 21 (11): 1953–60. https://doi.org/10.1681/ASN.2010020221.
Noori, Nazanin, Kamyar Kalantar-Zadeh, Csaba P. Kovesdy, Rachelle Bross, Debbie Benner, and Joel D. Kopple. 2010. “Association of Dietary Phosphorus Intake and Phosphorus to Protein Ratio with Mortality in Hemodialysis Patients.” Clinical Journal of the American Society of Nephrology : CJASN 5 (4): 683–92. https://doi.org/10.2215/CJN.08601209.
Ritz, Eberhard, Kai Hahn, Markus Ketteler, Martin K Kuhlmann, and Johannes Mann. 2012. “Phosphate Additives in Food—a Health Risk.” Deutsches Ärzteblatt International 109 (4): 49–55. https://doi.org/10.3238/arztebl.2012.0049.
Tonelli, Marcello, Frank Sacks, Marc Pfeffer, Zhiwei Gao, Gary Curhan, and Cholesterol And Recurrent Events Trial Investigators. 2005. “Relation between Serum Phosphate Level and Cardiovascular Event Rate in People with Coronary Disease.” Circulation 112 (17): 2627–33. https://doi.org/10.1161/CIRCULATIONAHA.105.553198.
Vaidya, Satyanarayana R., and Narothama R. Aeddula. 2025. “Chronic Kidney Disease.” In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK535404/. Wagner, Carsten A. 2023. “The Basics of Phosphate Metabolism.” Nephrology Dialysis Transplantation 39 (2): 190–201. https://doi.org/10.1093/ndt/gfad188.