Do you ever hear a sudden ringing in your ears that no one else does? You are not alone. In fact, roughly 10% of American adults experience this chronic condition called tinnitus (National Institute on Deafness and Other Communication Disorders (NIDCD), 2017). Tinnitus is often distressing as it disrupts focus and relaxation. To make matters worse, the frequency and severity of tinnitus seems to be rising during the SARS-CoV-2 pandemic. So what produces this bizarre condition?
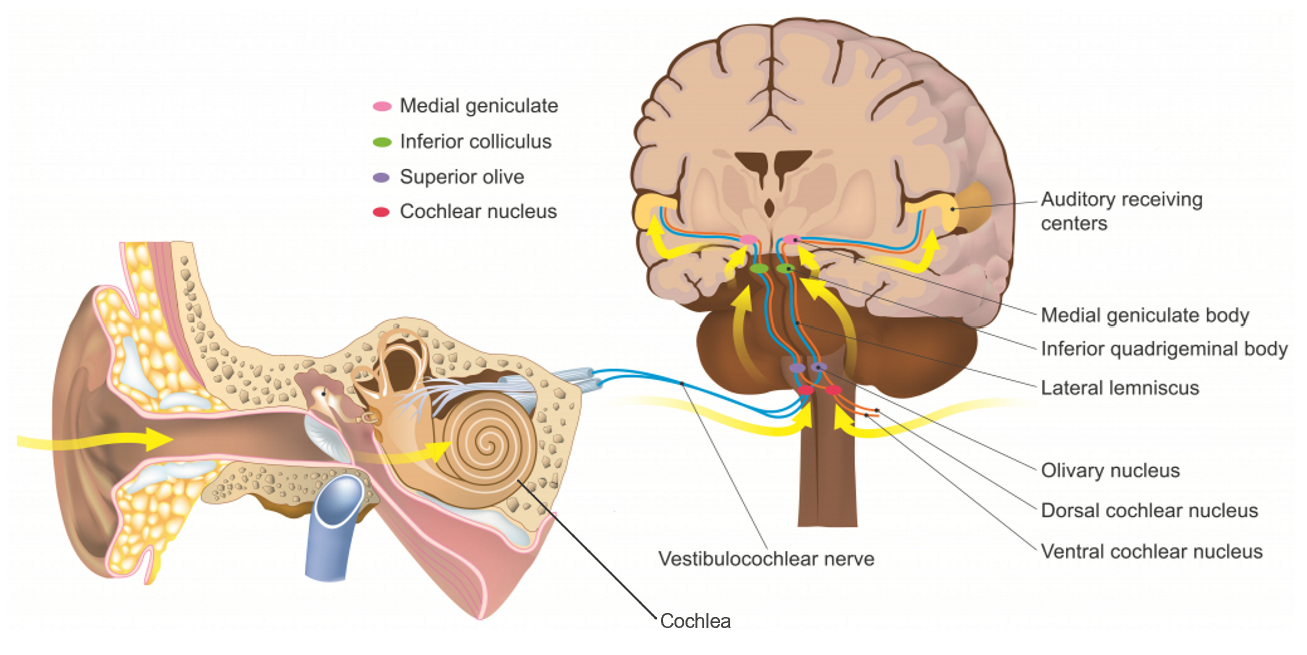
Unfortunately, there is no consensus on the cause of tinnitus. However, tinnitus and hearing loss often go hand in hand, suggesting that it occurs when hair cells in the cochlea become damaged. This would alter the transmission of signals along the auditory nerve to the brain, shown in Figure 1, causing a person to perceive sounds in absence of external stimuli—put simply, tinnitus (NIDCD, 2017). When cochlear hair cells are damaged, the brain may overcompensate by increasing the sensitivity of neurons making up the auditory nerve and the cochlear nuclei, which receive signals when the cochlear hair cells are stimulated by sound (Hébert et al., 2013). This increased neuron sensitivity could cause faint sounds to be perceived as loud ringing to people with tinnitus, while going unnoticed by everyone else. Tinnitus could also be caused by irregular interactions between neural circuits. The auditory system is closely intertwined with the limbic system, which manages mood and emotion. This link could substantiate correlations between tinnitus and increased stress (NIDCD, 2017; Ciminelli et al., 2018).

Jafari et al. reviewed evidence linking tinnitus to SARS-CoV-2, and they found a higher occurrence of tinnitus in people who had been infected (2021). However, little data was available describing details of the tinnitus, like pitch, loudness, and duration, which makes it hard to tell if the pandemic was really the cause. Still, the researchers propose that the immune system’s inflammatory response to SARS-CoV-2 contributes to this link. When the body detects SARS-CoV-2, it releases a multitude of inflammatory molecules that alert the immune system of the invading virus. Inflammation from SARS-CoV-2 may damage glial cells in the auditory system, leading to tinnitus (Jafari et al., 2021).
Alternatively, tinnitus may result from stress brought on by the pandemic. A 2020 study surveyed participants with tinnitus to ascertain whether illness, lifestyle changes, and emotional state influenced by SARS-CoV-2 impacted tinnitus symptoms (Beukes et al., 2020). The majority of participants with SARS-CoV-2 symptoms did not also experience increased tinnitus severity. However, heightened anxiety, sadness, and irritability resulting from the pandemic were linked to worsening tinnitus, suggesting that pandemic-related emotional stress is a contributing factor (Beukes et al., 2020).
There is no simple explanation for tinnitus, let alone for onset and worsening of symptoms during the pandemic. Tinnitus is especially challenging to study as a subjective experience which, in most cases, can only be detected through self-reporting. But maybe through detailed follow-up studies, researchers can learn more about possible links between tinnitus and SARS-CoV-2, providing new insight on both conditions.
Works Cited
Beukes, E.W., Baguley, D.M., Jacquemin, L., Lourenco, M.P.C.G., Allen, P.M., Onozuka, J., Stockdale, D., Kaldo, V., Andersson, G. and Manchaiah, V., 2020. Changes in Tinnitus Experiences During the COVID-19 Pandemic. Frontiers in Public Health, 8. https://doi.org/10.3389/fpubh.2020.592878.
Ciminelli, P., Machado, S., Palmeira, M., Carta, M.G., Beirith, S.C., Nigri, M.L., Mezzasalma, M.A. and Nardi, A.E., 2018. Tinnitus: The Sound of Stress? Clinical Practice and Epidemiology in Mental Health, 14(1). https://doi.org/10.2174/1745017901814010264.
Davies, K. and Sugano, Y., 2020. The Auditory Pathway. [image online] Available at: <https://teachmeanatomy.info/neuroanatomy/pathways/auditory-pathway/> [Accessed 25 March 2022].
Hébert, S., Fournier, P. and Noreña, A., 2013. The Auditory Sensitivity is Increased in Tinnitus Ears. Journal of Neuroscience, 33(6), pp.2356–2364. https://doi.org/10.1523/JNEUROSCI.3461-12.2013.
Jafari, Z., Kolb, B.E. and Mohajerani, M.H., 2022. Hearing Loss, Tinnitus, and Dizziness in COVID-19: A Systematic Review and Meta-Analysis. Canadian Journal of Neurological Sciences, 49(2), pp.184–195. https://doi.org/10.1017/cjn.2021.63.
National Institute on Deafness and Other Communication Disorders, 2017. Tinnitus. National Institutes on Health. Available at: <https://www.nidcd.nih.gov/health/tinnitus> [Accessed 25 March 2022].