
Pulse oximeters have revolutionized modern medicine, enabling continuous, accurate, and non-invasive monitoring of functional oxygen saturation of hemoglobin (SpO₂) (Chan et al. 2013). Taken as a fifth vital sign, the device’s use is routine in emergency care, general ward, intermediate/intensive care unit, the operating room, and in general practices (Bosch et al. 2024). However, with its prevalence in patient care and recent availability over the counter, the accuracy of the device has received critical attention, driven by the need to identify occult hypoxemia; a condition where a patient’s blood oxygen level is dangerously low, but a pulse oximeter reading incorrectly indicates it is within the normal range of greater than or equal to 92%(Cabanas et al. 2023). A critical factor affecting device accuracy is skin pigmentation, with large-scale studies and clinical reports documenting inaccuracies and overestimations in patients with higher skin melanin concentrations (Cabanas et al. 2023). These findings expose a deeper issue in healthcare: medical technologies and clinical practices designed and calibrated on lighter-skinned patients can perpetuate racial disparities, putting marginalized patients at higher risk of misdiagnoses, delayed treatment, and poorer healthcare outcomes.
A standard pulse oximeter determines oxygen saturation (SpO₂) by shining light at two or more wavelengths from a light-emitting diode through the tissue (typically the finger, and analyzing the resulting optical signals via a photodetector (Figure 1) (Cabanas et al. 2023; Chan et al. 2013).
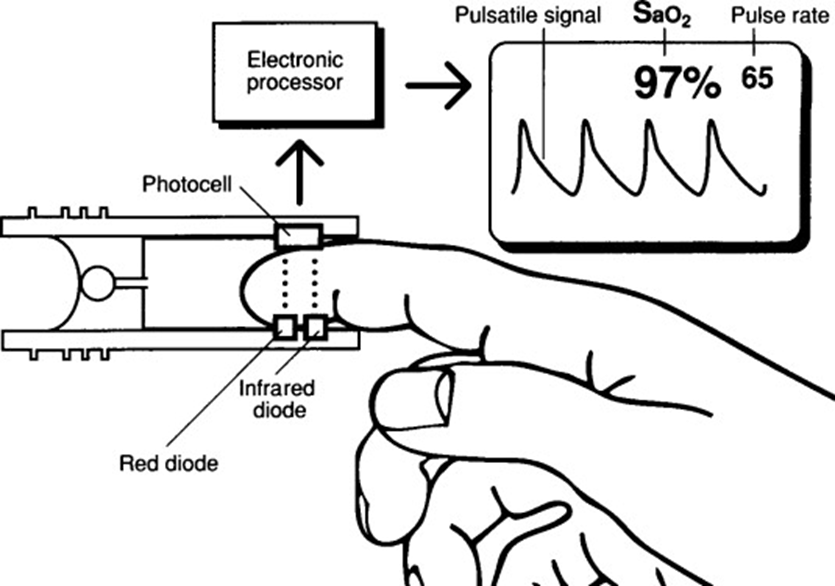
When the device illuminates a tissue site, the photodetector measures how much light is absorbed, generating two or more photoplethysmography signals. These signals fluctuate with the cardiac cycle: during systole, increased blood volume reduces the detected light, and during diastole, decreased blood volume increases detected light (Chan et al. 2013).
Wavelengths function based on the principle that oxyhemoglobin absorbs a greater amount of near-infrared (IR) light and lower amounts of red light than deoxyhemoglobin(Chan et al. 2013). This is why oxygenated blood appears bright red to the eye, as it transmits more red light, whereas deoxyhemoglobin absorbs more red light, appearing less red. Exploiting this difference in absorption patterns allows pulse oximeters to emit two wavelengths of light, red at 660nm and near-IR at 940nm. The transmitted light is then detected by a photodiode. By comparing the ratios of absorbed light at these two wavelengths, the pulse oximeter calculates the relative proportion of oxygenated hemoglobin in the blood, providing a continuous, real-time measurement of SpO₂.
However, because of the high light absorption capacity of melanin, the transmitted light wavelength is reduced, making the oximeter’s light unable to penetrate the subcutaneous tissue of patients with darker skin tones (Cabanas et al. 2023). This leads to systematic overestimation of SpO₂ in patients with higher melanin levels, as confirmed by clinical reports linking skin tone to diagnostic errors. For example, Sjoding et al. (2020) analyzed over 10,000 paired pulse oximetry and arterial blood gas measurements and found that Black patients were nearly three times more likely than white patients to have undetected hypoxemia (12% vs. 4%) despite “normal” SpO₂ readings. Similarly, Bickler et al. (2005) and Feiner et al. (2007) demonstrated that at true SpO₂ values below 90%, pulse oximeters overestimated oxygen saturation by up to 3–4% in individuals with darker pigmentation. These discrepancies can lead to missed diagnoses of hypoxemia in critical settings such as COVID-19 management, anesthesia, and neonatal care, where treatment thresholds are based on pulse oximetry readings (Fawzy et al. 2022). Emerging engineering solutions include advanced calibration with diverse skin tones, device redesign utilizing multi-wavelength sensing, and/or new light techniques like radially polarized light to reduce melanin’s interference with readings.
Overall, this disparity, which puts marginalized patients at risk of occult hypoxemia and delayed care, demands immediate, multi-faceted intervention to recalibrate devices and enforce equitable patient monitoring standards across all skin tones.
References
Bickler, Philip E., John R. Feiner, and John W. Severinghaus. 2005. “Effects of Skin Pigmentation on Pulse Oximeter Accuracy at Low Saturation.” Anesthesiology 102 (4): 715–19. https://doi.org/10.1097/00000542-200504000-00004
Bosch, Nicholas A., Anica C. Law, Ashraf Fawzy, and Theodore J. Iwashyna. 2024. “Prevalence of Inpatient Pulse Oximetry in Operative and Nonoperative Settings: A Multicenter Study.” CHEST Critical Care 2 (4): 100104. https://doi.org/10.1016/j.chstcc.2024.100104
Cabanas, Ana M., Pilar Martín-Escudero, and Kirk H. Shelley. 2023. “Improving Pulse Oximetry Accuracy in Dark-Skinned Patients: Technical Aspects and Current Regulations.” British Journal of Anaesthesia 131 (4): 640–44. https://doi.org/10.1016/j.bja.2023.07.005
Chan, Edward D., Michael M. Chan, and Mallory M. Chan. 2013. “Pulse Oximetry: Understanding Its Basic Principles Facilitates Appreciation of Its Limitations.” Respiratory Medicine 107 (6): 789–99. https://doi.org/10.1016/j.rmed.2013.02.004
Chandraguptha, Dilshan. 2021. “Pulse Oximetry.” FOS Media Students’ Blog, September 4. https://fos.cmb.ac.lk/blog/pulse-oximetry/.
Fawzy, Ashraf, Tianshi David Wu, Kunbo Wang, et al. 2022. “Racial and Ethnic Discrepancy in Pulse Oximetry and Delayed Identification of Treatment Eligibility Among Patients With COVID-19.” JAMA Internal Medicine 182 (7): 730. https://doi.org/10.1001/jamainternmed.2022.1906
Feiner, John R., John W. Severinghaus, and Philip E. Bickler. 2007. “Dark Skin Decreases the Accuracy of Pulse Oximeters at Low Oxygen Saturation: The Effects of Oximeter Probe Type and Gender.” Anesthesia & Analgesia 105 (6): S18–23. https://doi.org/10.1213/01.ane.0000285988.35174.d9
Sjoding, Michael W., Robert P. Dickson, Theodore J. Iwashyna, Steven E. Gay, and Thomas S. Valley. 2020. “Racial Bias in Pulse Oximetry Measurement.” New England Journal of Medicine 383 (25): 2477–78. https://doi.org/10.1056/NEJMc2029240
Comments
7 Responses to “Skin Pigmentation Bias in Pulse Oximetry Measurements”
Hey iSci,
I decided to write this blog post because it is (unfortunately) a very prevalent issue to date. I wanted to delve more deeply into the mechanisms behind pulse oximetry, and found a lot of the concepts related to key light and absorption properties explored in physics. This post integrated some technical aspects of pulse oximetry devices and, more importantly, how these devices put certain patients at risk.
I hope you find this issue as alarming and urgent as I do. Please give me as much feedback as possible!
Thanks,
Leah
Hi Leah,
I really enjoyed your post! The topic is very relevant, and I like how you raised awareness while also integrating physics and neuroscience themes. I just have a few suggestions that I hope will be helpful for the final copy!
-Make sure to remove the comma in the last in-text citation of paragraph 5. The citation should read like this: (Fawzy et al. 2022; FDA 2024).
-In your reference list, the Commissioner’s Office source is listed as 2025, but in the text, you cite it as FDA 2024. I recommend verifying the correct publication year. Also, the hyperlink for this source appears to be broken, so you may want to update it.
-You don’t need to introduce accronyms for LED and PPG since they are never used again in the text.
-Be sure to reference your figure somewhere in the text. You could do this in the paragraph directly above it when you briefly explain how pulse oximeters work.
Overall, I really enjoyed reading your blog post and it was very well written! I hope these suggestions were helpful.
Happy editing!
Kristen
Hi Kristen,
Thank you so much for your helpful feedback! I will make sure to implement your suggestions.
Thanks,
Leah
Hi Leah!
This was a really informative post on an important issue that people may not know prevails in our medical industry, here are some suggestions for you to consider:
– P1S4: ‘Overestimates’ might not be the right version of the word here, ‘overestimations’ should be a better fit.
– P2S2: You have a period before your citation you should probably delete.
– Figure 1: Well written figure description! You should consider referencing it in the text above it since you’ve included it.
– P3S1: If you have a word you only use the abbreviations of once you don’t need to include it such as PPG and O2Hb (consider removing HHB).
– P3S1: For grammar, it could be better to say either ‘A wavelength functions based on…’ or ‘Wavelengths function based…’
Happy editing :))
Fiona
Hi Fiona!
Thanks for all your helpful feedback and catching those mistakes! I will make sure to implement your suggestions.
Thanks,
Leah
Hi Leah,
This was an awesome blog post!!
Here is some feedback:
-In your first sentence, I like how you explain what pulse oximeters are, but I wonder if you could more clearly say what SaO2 is?
-In your third sentence, maybe explain why occult hypoxemia is bad or some symptoms associated with it. Just by seeing the defined arterial oxygen saturation <88% I don’t know really why I should be concerned. You could also say what the normal healthy pecentage is to provide a comparison.
-You don’t need an in text citation at the end of the fourth sentence since you used the same source in the previous sentence.
-What specifically is SpO2?
-Be consistent with O₂ vs. O2
Overall this was an awesome post and a very important topic! I learned a lot.
Happy editing,
Emma
Hi Emma,
Thank you for your helpful feedback! I see where some further clarification is required, and I’m glad you brought up these points! I’ll make sure to implement your suggestion for my final draft.
Thanks,
Leah