The ongoing opioid epidemic continues to be a public health concern in Canada and many other parts of the world, fuelled by both prescription and illegally obtained opioids (Belzak and Halverson 2018). Naloxone, generally known by its brand name Narcan, is the most commonly used medication that is administered during opioid overdose emergencies (Theriot et al. 2025). It acts as an opioid antagonist that works against drugs such as morphine, oxycodone, heroin, and fentanyl (Sirohi et al. 2009). It is important to note that naloxone is not effective against non-opioid stimulants such as cocaine, methamphetamine, and benzodiazepines (PubChem 2025). Naloxone has a high affinity for μ-opioid receptors in the ventral tegmental area of the brain, making them the primary target for pain-relieving drugs (Theriot et al. 2025). By binding to these receptors, naloxone helps to temporarily reverse the effects that opioids have on the body such as arrested respiration, respiratory and central nervous system (CNS) depression, apnea, unconsciousness, and miosis (Saari et al. 2024). The efficacy of naloxone is dependent on several factors, which include the dose of the opioid that is ingested, the pharmacological mechanism of the opioid, as well as the medical history of the victim (Jordan et al. 2025).
The chemical formula of naloxone is C19H21NO4, with a molecular weight of approx. 327.38 g/mol (PubChem 2025). It is a congener of oxymorphone, differing by only an allyl group that reverses the effect of the opioid ingested. Narcan is chemically formulated as naloxone HCl, the hydrochloride salt form of naloxone that enhances stability, solubility, and bioavailability (Wermeling 2013). Due to its lipophilic nature, naloxone is able to cross the blood-brain barrier within 2 minutes of being administered, to bind to the μ-opioid receptor’s orthosteric site, where it displaces the opioid molecule (Moss and Carlo 2019). This displacement prevents G-protein activation, thereby increasing the activity of adenylyl cyclase and restoring cyclic Adenosine Monophosphate (cAMP) production in the neurons.
Restored cAMP levels lead to the reopening of voltage-gated calcium channels and normal neuronal activity (figure 1). In the brainstem, this restores respiration, reversing opioid-induced respiratory depression. After its action in the CNS, naloxone is metabolized in the liver and is excreted through the kidneys (Moss and Carlo 2019).
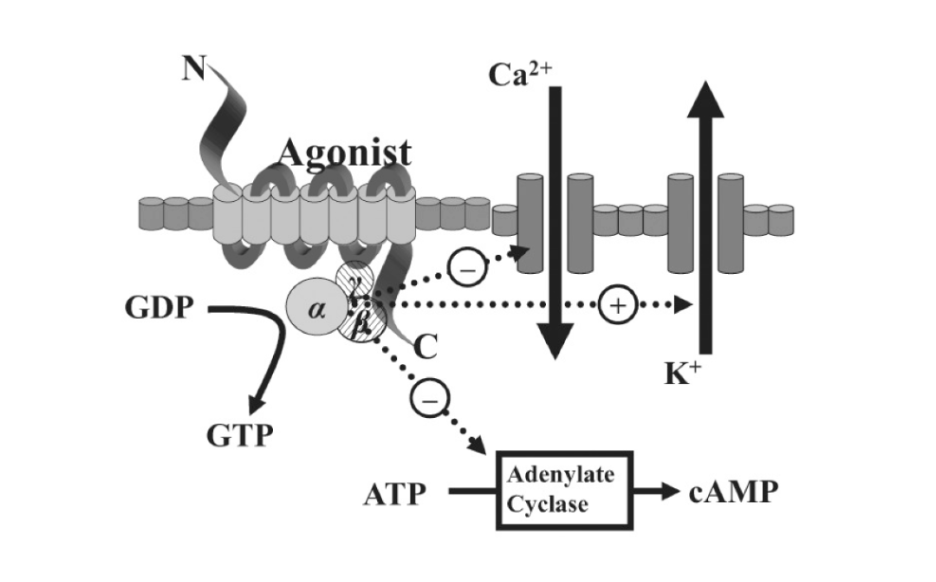
Figure 1. Cell signaling cascade of the binding of an opioid agonist. This figure illustrates how opioid receptor activation inhibits adenylate cyclase, reducing cAMP, suppressing calcium entry, and upregulating potassium efflux from the neuron. This leads to a decline in neuronal excitability and neurotransmitter release, which controls the pain-relieving effects of opioids. Naloxone blocks the opioid from the receptor, preventing G-protein activation, which leads to the restoration of respiratory function (Pathan and Williams 2012).
The Food and Drug Administration (FDA) approved of the parenteral (injectable) use of naloxone in 1971, which made its way into clinics, hospitals, and prehospital medicine settings (Saari et al. 2024). However, intranasal naloxone was approved for use by the FDA in 2015 (Jenco 2023). This was primarily done to allow general members of the public such as social workers, family members, residents of high-risk communities to able to administer naloxone efficiently, in response to the rising rates of opioid-related deaths and overdoses (Urmanche and Harocopos 2023). In Canada, there is an Increased availability of naloxone to enforce extra precautions that can be taken regarding the opioid epidemic (Tsuyuki et al. 2020). Enacted policies now allow first responders including firefighters to carry naloxone, and it is freely available at local pharmacies. In some provinces, pharmacies are also required to provide a naloxone kit when patients are prescribed opioids (Government of Ontario 2023).
Naloxone has proven to serve as a critical, fast acting opioid antagonist that can effectively reverse life-threatening symptoms of overdose by restoring normal respiratory and neurological function. Its widespread availability has made it an essential public health tool in controlling and mitigating the devastating impact of the opioid epidemic.
References
Belzak, Lisa, and Jessica Haverson. 2018. “Evidence Synthesis – The Opioid Crisis in Canada: A National Perspective.” Health Promotion and Chronic Disease Prevention in Canada: Research, Policy and Practice 38 (6): 224–33. https://doi.org/10.24095/hpcdp.38.6.02
Government of Ontario. 2023. “Ontario Take-Home Naloxone Programs | Ontario.Ca.” November 2. https://www.ontario.ca/page/ontario-take-home-naloxone-programs
Jenco, Melissa. 2023. AAP Expert: FDA Approval of OTC Naloxone Nasal Spray Is a ‘Win.’ March 30. https://publications.aap.org/aapnews/news/23940/AAP-expert-FDA-approval-of-OTC-naloxone-nasal.
Jordan, Matthew R., Preeti Patel, and Daphne Morrisonponce. 2025. “Naloxone.” In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK441910/.
Moss, Ronald B., and Dennis J. Carlo. 2019. “Higher Doses of Naloxone Are Needed in the Synthetic Opioid Era.” Substance Abuse Treatment, Prevention, and Policy 14 (1): 6. https://doi.org/10.1186/s13011-019-0195-4.
Pathan, Hasan, and John Williams. 2012. “Basic Opioid Pharmacology: An Update.” British Journal of Pain 6 (1): 11–16. https://doi.org/10.1177/2049463712438493.
PubChem. 2025. “Naloxone.” Accessed October 12, 2025. https://pubchem.ncbi.nlm.nih.gov/compound/5284596.
Saari, Teijo I., John Strang, and Ola Dale. 2024. “Clinical Pharmacokinetics and Pharmacodynamics of Naloxone.” Clinical Pharmacokinetics 63 (4): 397–422. https://doi.org/10.1007/s40262-024-01355-6.
Sirohi, Sunil, Shveta V. Dighe, Priyanka A. Madia, and Byron C. Yoburn. 2009. “The Relative Potency of Inverse Opioid Agonists and a Neutral Opioid Antagonist in Precipitated Withdrawal and Antagonism of Analgesia and Toxicity.” The Journal of Pharmacology and Experimental Therapeutics 330 (2): 513–19. https://doi.org/10.1124/jpet.109.152678.
Theriot, Jonathan, Sarah Sabir, and Mohammadreza Azadfard. 2025. “Opioid Antagonists.” In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK537079/.
Tsuyuki, Ross T., Vinita Arora, Mark Barnes, et al. 2020. “Canadian National Consensus Guidelines for Naloxone Prescribing by Pharmacists.” Canadian Pharmacists Journal / Revue Des Pharmaciens Du Canada 153 (6): 347–51. https://doi.org/10.1177/1715163520949973.
Urmanche, Adelya A., and Alex Harocopos. 2023. “Experiences Administering Naloxone Among People in Different Social Roles: People Who Use Opioids and Family Members and Friends.” Journal of Drug Issues 53 (3): 475–89. https://doi.org/10.1177/00220426221133024.
Wermeling, Daniel P. 2013. “A Response to the Opioid Overdose Epidemic: Naloxone Nasal Spray.” Drug Delivery and Translational Research 3 (1): 63–74. https://doi.org/10.1007/s13346-012-0092-0.
Comments
16 Responses to “What is Naloxone – and More Importantly, How Does It Work? ”
Hello iSci,
I decided to write about naloxone because a family member of mine was given an opioid prescription from the doctor’s office, and when they went to the pharmacy to pick it up, they were also handed a naloxone kit. I was curious about how it worked, so I did some research on it. I also wrote about this topic to bring awareness to the ongoing opioid crisis.
I am open to suggestions, happy reading!
Hi Tinu!
This was such an informative read. I’ve heard of Narcan before but I never knew how it worked. As for suggestions, I think that this was really well written and dense with information which is a good thing. The only thing I can say which is VERY nitpicky, is that in your first sentence, you spelled “fueled”, which technically isn’t incorrect but would be more correct if you spelled it as fuelled, since that’s the Canadian version.
Happy editing!
Afua
Hello Afua,
Thank you for reading my blog post and I am glad you found it insightful. I have changed “fueled” to “fuelled” as per the Canadian version.
– Tinu
Hello Tinu,
Great job on your post! I thought your writing was super engaging and the topic you chose was very fascinating.
One suggestion I have is to potentially include any immediate body side effects after naloxone use (like nausea and body aches) occuring due to opioid withdrawel. Adding this could be beneficial to highlight the severity of the crisis by detailing the severe physical risks from opioid dependency.
Overall, very well done!
Thanks,
Seanna
Hello Seanna,
Thank you for reading my blog post!
Your suggestion is definitely an important aspect to consider, but I do not have the space to include additional information as I am also within my 10% buffer.
Thank you once again.
– Tinu
Hi Tinu!
I loved reading your blog post, I’ve seen signs in pharmacies about naloxon and wondered what it was.
A suggestion I have is in the first paragraph you mention that the “ventral tegmental area of the brain”, it might be helpful to include a figure of the brain indicating where the naloxone targets.
Happy editing!!
Emily
Hello Emily,
Thank you for your suggestion, I decided not to include a figure referring to the ventral tegmental area of the brain because while it would be a helpful guide for readers, the focus of my topic is on the social/physiological aspects of naloxone. I would also need to provide some context for the figure as well, which I do not have the space for.
Thank you for reading my blog, and i am glad that you enjoyed it.
Hello Tinu,
This was such an interesting post! I love how you connected the complex science behind naloxone to the larger public health context of the opioid crisis.
I think adding a short explanation of how naloxone interacts with the brain’s receptors (maybe highlighting the ventral tegmental area you mentioned) could help readers understand what’s happening at a molecular level (only if word count permits 🙂 )
You could also consider breaking up the longer middle paragraph so the pharmacology part reads more smoothly.
Overall, your writing is super clear and informative.
Happy editing 🙂
Hey Hana,
Thank you for your helpful feedback. I broke up my middle paragraph, hopefully it flows better now.
Thank you for reading my blog, I am glad that you enjoyed it.
– Tinu
Hi Tinu,
I really enjoyed reading your post, it was super interesting. All my suggestions are pretty minor.
First, I would recommend hyperlinking your sources on your reference page to make it easier for the reader to access them. I also noticed that P1S2 and P2S4 contain ” μ-opioid” which formatted weirdly for me on my computer, but I have not seen any other comments about it so maybe it’s just me (incase you’re curious here’s a google doc with a screenshot of the issue: https://docs.google.com/document/d/1A7M8Jyb3dRORlBUVjgWn4E4JF7eRmgC-lEZJ8eBrV0g/edit?usp=sharing).
Overall, I think your post is fantastic, and I hope you had fun writing it.
Charlie
Correction: it is in P1S5, sorry about that
Hello Charlie,
Thank you for helpful suggestions, I have made the necessary changes.
– Tinu
Hi Tinu,
This was a really interesting and informative post!
A few suggestions:
– There are a few words in the middle of sentences that are capitalized that shouldn’t be
– The chemical formula of hydrogen chloride/hydrochloric acid is “HCl” rather than “HCL”
– I’d suggest including a figure that shows the structure of naloxone instead of the formula since there are numerous isomers in the case of a molecule with so many atoms. I also don’t think you need to include the molecular weight since it doesn’t seem very relevant to your post.
Overall, a great read!
Best,
Riley
Hello Riley,
Thank you for helpful suggestions, I have made the necessary changes.
I am glad you found my blog interesting.
– Tinu
Hi Tinu,
Great blog post! I learned a lot and I definitely think this is a very relevant and impactful topic. With that in mind, I had a few comments:
– I would double check your citation “PubChem. n.d. “Naloxone.” Accessed October 12, 2025. https://pubchem.ncbi.nlm.nih.gov/compound/5284596.”.
On this website, they have a few citation examples of how to cite it, including APA:
“National Center for Biotechnology Information (2025). PubChem Compound Summary for CID 5284596, Naloxone. Retrieved October 27, 2025 from https://pubchem.ncbi.nlm.nih.gov/compound/Naloxone.”
I would just take a look and maybe format yours accordingly in iSci format.
– In your conclusion or in your piece it might be interesting to think about public health implications. I believe in the US, the government is reducing funding for Narcan training programs: https://www.cbsnews.com/news/overdose-deaths-narcan-naloxone-harm-reduction-samhsa-trump-cuts/. If you have the space, it could be interesting to discuss this and your take on it.
– Remember to hyperlink your sources.
Overall, great post! I learned a lot and enjoyed.
Happy editing,
Siya
Hello Siya,
Thank you for taking the time to read my blog post. I have made the necessary changes.
I am glad you found it interesting.
– Tinu